
Ketogenic diet is a high fat, low carbohydrate and normal protein diet. The most common myth about using KD is that this diet could lead to nutritional deficiencies. It is believed that because it is a low carbohydrate diet, it is deficient in major nutrients as fruits and vegetables are limited.
But that is not true. At our center, we believe that ‘prevention is better than cure’. So KD is supported by all necessary supplements such multivitamins, minerals like calcium, iron zinc selenium etc.
All patients are given preventive supplements such as multivitamin and multi-mineral tablets, calcium and potassium citrate. Other supplements are added if there is a need, for example, patients who have carnitine or iron deficiency.
The table below show the role of these supplements:
| Supplements( Vitamins and Minerals) | Health benefits |
| Multivitamin | To prevent various nutritional deficiencies. |
| Calcium | To prevent growth retardation in children.
To prevent bone diseases in adult |
| Vitamin D | To prevent growth retardation and bone diseases in adult |
| Potassium citrate* | To prevent Kidney stones (McNally et al, 2009) |
| Iron | To prevent anemia |
Studies showing importance of supplements while on KD:-
Ketogenic diet and trace minerals ( Zinc and Selenium)
The ketogenic diet is deficient in several trace minerals, and if children are maintained on the diet for more than 2 years, these need to be supplemented. (Bergqvist AGC et al, 1999; Chee CM et al, 1998)
Zinc deficiency is closely associated with stunting, respiratory infections, diarrhea, and dermatitis.
Zinc deficiency also leads to loss of taste therefore affecting appetite. Zinc deficiency has been linked to a diminished sense of taste in rats and in humans who were made zinc deficient experimentally.
Several patients who presented with idiopathic hypogeusia, dysgeusia, hyposmia, and dysosmia {A reduction in taste sensitivity (hypogeusia), an absence of taste sensation (ageusia), or a distortion of normal taste (dysgeusia)} were empirically treated with zinc sulfate orally, and within a short time their symptoms diminished and their hypogeusia improved.
In uncontrolled clinical studies, the administration of zinc has been reported to correct abnormalities of taste in cancer patients who had received ERT to the head and neck region over the previous 1 year. (Ripamonti et al,1998)
More recently, selenium deficiency was found in nine children on the ketogenic diet, including one who developed cardiomyopathy (Bergqvist et al, 2003).
*Ketogenic diet and Potassium citrate:-
For nearly a century, the ketogenic diet (KD) has been recognized as an effective non-pharmacologic treatment for epilepsy. Despite positive effects on seizure frequency, repeated studies have shown that the KD is associated with an increased prevalence of kidney stones, ranging from 3–6% over a typical 2 year diet duration. Hypercalciuria, urine acidification, and hypocitraturia, all known risk factors for kidney stones, often occur in patients on the KD.
Oral potassium citrate is an effective preventative supplement against kidney stones in children receiving the KD, achieving its goal of urine alkalinization. Universal supplementation is warranted (McNally et al, 2009)
Ketogenic diet and Carnitine :-
Carnitine is important while on the ketogenic diet because the high fat intake means more fatty acids need to be transported into the mitochondria for oxidation, requiring more carnitine and therefore increasing the risk of depleting of body carnitine stores (Berry-Kravis et al, 2001)
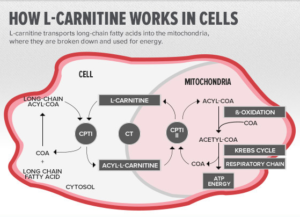
Carnitine, a branched non-essential amino acid, is synthesized from the essential amino acids lysine and methionine. It was originally labeled vitamin BT; however, because carnitine is synthesized in the human body, it is no longer considered a vitamin. It is an essential nutrition in our body that transports long chain fatty acids across the mitochondrial membrane to turn fat into energy.
Fatty Acid Oxidation
Though fatty acids are one of the primary energy sources for the body, they cannot produce energy until they are broken down in mitochondria (the ‘furnace’ or ‘power-house’ of the cell) through a process called, ß-oxidation. This is where L-Carnitine plays an essential role to complete the process since fatty acids alone cannot penetrate the inner mitochondrial membrane and enter the mitochondria for subsequent fat breakdown and energy production. (Flanagan et al, 2010)
Now let us see how these Nutrients are beneficial in ketogenic diet in treating neurological disorders.
As we are using ketogenic diet exclusively for treating epilepsy patients. Let’s first understand the role of Nutritional supplements in Epilepsy:-
Nutrients that may reduce seizure frequency include vitamin B6, magnesium, vitamin E, manganese, taurine, dimethylglycine, and omega-3 fatty acids. Administration of thiamine may improve cognitive function in patients with epilepsy. Supplementation with folic acid, vitamin B6, biotin, vitamin D, and L-carnitine may be needed to prevent or treat deficiencies resulting from the use of anticonvulsant drugs (Gaby AR, 2007)
| Nutrients | Cause of deficiency | Benefits | References |
| Vitamin B6 | Low levels of vitamin B6 may be due in part to treatment
with phenytoin.
| One practitioner found that supplementation
with 600 mg/day vitamin B6 reversed phenytoin-induced gingival hyperplasia in several patients | |
| Magnesium | Severe magnesium depletion can cause seizures or increase susceptibility to seizure-inducing
stimuli. | Oral administration
of magnesium has been associated in some cases with an improvement in EEG findings and a reduction in seizure frequency. | |
| Vitamin E | Vitamin E levels were lower in children
receiving multi-drug therapy | Although the research on efficacy is conflicting,
vitamin E is relatively safe and may be considered for adjunctive treatment in epileptic patients, particularly children. | |
| Manganese | In humans with epilepsy, whole-blood manganese
levels were significantly lower by 20-41 percent than in controls. In rats, manganese deficiency increased susceptibility to electroshock-induced convulsions. | Manganese
deficiency is a primary contributing factor, rather than a consequence, of epilepsy or its treatment. | |
| Folic Acid | Seizures occur in some infants with cerebral
folate deficiency, a syndrome that also includes slow head growth, psychomotor retardation, cerebellar ataxia, and other neurological abnormalities. Folate deficiency is due primarily to the use of anticonvulsant medications (e.g., phenytoin, valproate, carbamazepine, phenobarbital, and primidone), which interfere with folic acid absorption.
| Folic acid has also been used to treat phenytoin
-induced gingival hyperplasia. | |
| Biotin | Low biotin levels appear to result
from an acceleration of biotin catabolism by phenytoin, carbamazepine, and phenobarbital | Correction of biotin deficiency might reduce
seizure frequency, as suggested by the fact that biotin responsive seizures have occurred in some patients with inborn errors of biotin metabolism | |
| Vitamin D | Patients taking anticonvulsants are at increased
risk of developing vitamin D deficiency, apparently because these drugs induce liver enzymes that inactivate vitamin D. | ||
| Essential Fatty Acids | Supplementation with fish oil (providing
1 g/day EPA and 0.7 g/day DHA) reduced seizure frequency | ||
| Carnitine | An additional risk in some individuals is that long term use of the medication sodium valproate also can lead to carnitine deficiency. If carnitine is deficient, it will be difficult to achieve adequate ketosis on the ketogenic diet, due to impaired ketone body synthesis; energy levels may also be impaired. | Anecdotal reports do suggest ketone levels may improve with additional carnitine supplementation. |
A number of different dietary modifications, nutritional supplements, and hormones may help prevent seizures or improve other aspects of health in patients with epilepsy. Supplementation with specific nutrients should also be considered for the prevention and treatment of nutritional deficiencies resulting from anticonvulsant drugs.
Nutrient supplement and Other Neurological disorders
Vitamin D and Multiple sclerosis:-
Ascherio et al, 2014 suggested that identification and correction of vitamin D insufficiency has an important role in the early treatment of MS.
Multiple sclerosis (MS) is a common cause of neurological disability in young adults.
A higher MS risk in individuals with low vitamin D intake 3 or low circulating 25-dihydroxyvitamin D (25(OH)D) as well as an inverse correlation between vitamin D status and MS activity have been reported and suggest that vitamin D is related to the disease process that leads to and perpetuates MS.
Magnesium and Anxiety disorder (In Parkinson disease):-
Combination nutritional supplements containing lysine or magnesium also appear to hold promise as treatments for anxiety symptoms and disorders.( Lakhan and Vieira Nutrition Journal 2010, 9:42)
Multivitamin and Alzheimer’s’
These findings indicate that in the elderly, multivitamin supplementation may enhance neural efficiency during memory retrieval (Macpherson H, 2012)
Antioxidant ( Vitamin E and Vitamin C) and Alzheimer disease:-
Antioxidants may protect the aging brain against oxidative damage associated with pathological changes of Alzheimer disease (AD). Use of vitamin E and vitamin C supplements in combination is associated with reduced prevalence and incidence of AD. Antioxidant supplements merit further study as agents for the primary prevention of AD (Zandi PP et al, 2004)
Multivitamin and Cancer
Thorne RN et al (1994) reported a decline in the incidence of medulloblastoma. In a recent case control study, a protective effect of maternal folate, iron, and multivitamin supplementation against primitive neuroectodermal tumors, including medulloblastoma was found.
The introduction of periconceptional multivitamin supplementation in the 1980s may have caused this significant decline in the incidence of medulloblastoma.
Essential fatty acid and Dementia:-
Nutrition may be relevant to the pathogenesis of dementia through many processes. Higher intake of energy and lower intake of antioxidants may exaggerate the process of dementia through oxidative stress. Excessive amounts of n-6 PUFA or deficiency of n-3 PUFA may cause chronic inflammation, platelet aggregation, or endothelial dysfunction of microvasculature. Nutrition may be useful for preventing dementia, although gender-specific differences must be taken into account.(Otsuka M et al, 2002)
Attention is directed to the fact that the ketogenic diet is much less toxic than some of the medications currently used in the treatment of epilepsy. (Dr Samuel Livingston, 1972)
The ketogenic diet is an effective and safe medical treatment for epilepsy, but it must be judiciously applied and carefully monitored. (Drs Doug R. Nordli and Daryl C. DeVivo, 2001)
So to make ketogenic diet a balanced diet, you need to support it with nutritional supplement as recommended by expert doctors and dieticians.
We would also like to share the dietary sources of the nutrients mentioned in this section:-
| Nutrient | Sources |
| Carbohydrate & fibre | Whole meal bread, wholegrain cereals, baked beans, pasta, potatoes, peas, other starchy vegetables |
| Protein | Lean meat, chicken, fish, cheese, milk, eggs, nuts, legumes |
| Fat | Oils, butter, margarine, cream, meat, cheese, pastry, biscuits, nuts |
| Beta-carotene (converts to vitamin A) | Carrots, spinach, pumpkin, broccoli, tomatoes, apricots, rockmelon |
| Vitamin D | Vitamin D-fortified milk. In addition, exposure to sunlight is another source of Vitamin D. Of all the other nutrients, Vitamin D is produced in the skin with stimulus of sun. |
| Vitamin E | Polyunsaturated oils, polyunsaturated margarine, nuts, olive oil, fatty fish and small amounts in wholegrain cereals and green vegetables |
| Vitamin K | Green vegetables, milk, meat, pork, eggs |
| Thiamin | Wholegrain cereals, pork, bread, nuts, peas |
| Riboflavin | Milk, meat, eggs, cheese, wholegrain, cereals, nuts, mushrooms |
| Niacin | Fish, meat, peanuts, wholegrain cereals, nuts, mushrooms |
| Pantothenic acid | Eggs, wholegrain cereals, peanuts, fish, meat, vegetables |
| Vitamin B6 | Wholegrain cereals, meat, fish |
| Folic acid | Green vegetables, wholegrain cereals, whole meal bread, nuts, flour, corn meal, pasta, rice and other grain products; vegetables; mustard and turnip greens; liver; citrus fruit juices; and legumes. |
| Vitamin B12 | Meat, fish, eggs, cheese, milk, oysters |
| Biotin | Liver, kidneys, egg yolk, eggs, cheese, milk, fish, wholegrain cereals |
| Vitamin C | Oranges, tomatoes, potatoes, broccoli, cabbage, Brussels sprouts, Strawberries, cantaloupe, grapefruit, grapefruit juice, honeydew melon, kiwi fruit, mandarin orange sections, mango, orange juice, papaya, strawberries, tangerines, asparagus, broccoli, brussels sprouts, cabbage, cauliflower, kale, sweet green and red peppers, sweet potatoes. |
| Calcium | Cheese, milk, yoghurt, canned fish, nuts, sesame seeds (tahini), dried fruit |
| Phosphorus | Meat, fish, poultry, eggs, milk, cheese, nuts, cereals, bread |
| Iron | Meat, poultry, wholegrain cereals, wholemeal bread, eggs |
| Sodium | Table salt, meat, milk, cheese, seafood, spinach, celery |
| Potassium | Potatoes, bananas, oranges, apricots, other fruit and vegetables, meat, fish, nuts |
| Iodine | Sea foods, milk and cereals and vegetables from areas with high iodine content in the soil, iodised table salt |
| Zinc | Oysters, meat, fish, poultry, eggs, wholegrain cereals, peanuts |
| Magnesium | Green leafy vegetables, nuts (including brazil nuts, almonds, and cashews), meats, beef liver, salmon, cheddar cheese, milk, eggs, and dry beans and peas. |
| Manganese | Nuts, rice, whole grains, beans, and leafy green vegetables. |
| Selenium | Fish, organ meats, shellfish, eggs, and grains and plants grown in selenium-rich soil. |
References:-
- McNally et al. Empiric use of Oral Potassium Citrate Reduces Symptomatic Kidney Stone Incidence with the Ketogenic Diet. 2009 August ; 124(2): e300–e304.
- Flanagan et al. Review Role of carnitine in disease. Nutrition & Metabolism 2010, 7:30.
- Chee CM, Lutchka L, Brown L, et al: Ketogenic diet: Unrecognized selenium deficiency, abstract. Epilepsia 1998;39(Suppl 6):228.
- Ripamontiet ZincSulfateinTreatingTasteAlterations.CANCERMay15,1998/Volume82/Number1
- Bergquist AGC, Chee CM, Lutcha L, Rychik J, Stallings VA (2003). Selenium deficiency associated with cardiomyopathy: a complication of the ketogenic diet. Epilepsia 44(4):618-620.
- Bergqvist AGC, Chee CM, Bettler JE, et al: Zinc deficiency resulting from the ketogenic diet, abstract. Epilepsia 1999;40(Suppl 7):133.
- Berry-Kravis et al (2001). Carnitine levels and the ketogenic diet. Epilepsia42 (11), 1445-1451.
- Gaby AR. Natural approaches to epilepsy. Altern Med Rev. 2007 Mar;12(1):9-24.
- Ascherio et al.Vitamin D as an early predictor of multiple sclerosis activity and Progression JAMA Neurol. 2014 March ; 71(3): 306–314.
- Lakhan and Vieira. Nutritional and herbal supplements for anxiety and anxiety-related disorders: systematic review. Nutrition Journal 2010, 9:42
- Macpherson H et al. Neurocognitive effects of multivitamin supplementation on the steady state visually evoked potential (SSVEP) measure of brain activity in elderly women. Physiol Behav. 2012 Oct 10;107(3):346-54.
- Zandi PP et al. Reduced risk of Alzheimer disease in users of antioxidant vitamin supplements: the Cache County Study. Arch Neurol. 2004 Jan;61(1):82-8.
- Thorne RN et al. Decline in incidence of medulloblastoma in children. Cancer. 1994 Dec 15;74(12):3240-4
- Otsuka M et al. Similarities and differences between Alzheimer’s disease and vascular dementia from the viewpoint of nutrition. Ann N Y Acad Sci. 2002 Nov;977:155-61
- Livingston S: Dietary treatment of epilepsy, in Livingston S (ed): Comprehensive Management of Epilepsy in Infancy, Childhood and Adolescence. Springfield, IL, Charles C. Thomas, 1972, 378-405.
- Nordli DR, DeVivo DC: The ketogenic diet, in Wyllie E (ed): The Treatment of Epilepsy: Principles and Practice, 3rd ed. New York, Lippincott, Williams & Wilkins, 2001, 1001-1006.